People with ME/CFS do not need to be convinced of the reality of the disease – they live with its impact day in and day out. Nevertheless, disbelief and misunderstanding remain common, making research that demonstrates the biological nature of the illness particularly valuable.
Can understanding symptom clusters in ME/CFS provide further validation?
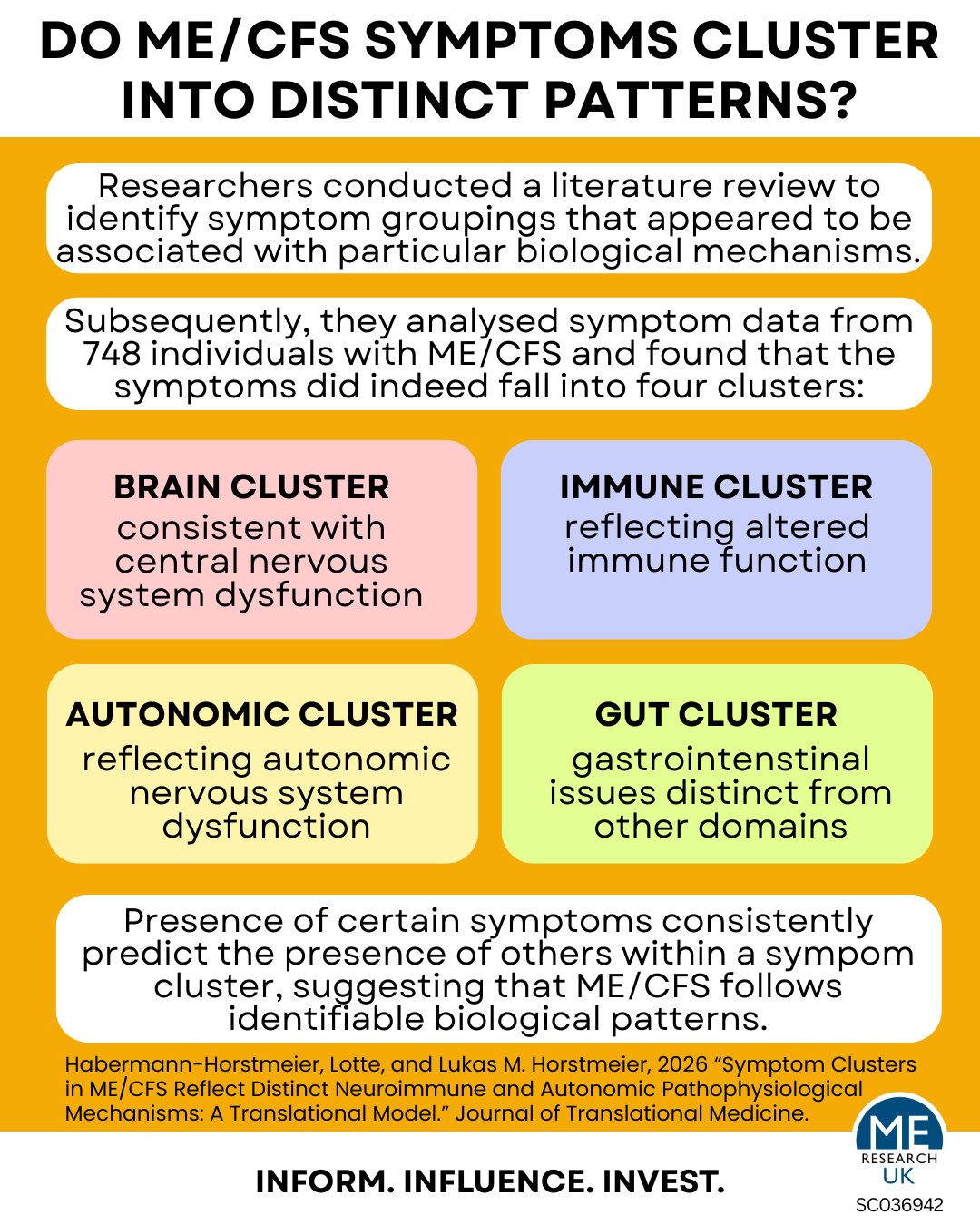
In a recent study, researchers set out to test a specific idea – that the extensive range of symptoms experienced by people with ME/CFS is not random. They hypothesised that symptoms would cluster together in highly predictable patterns according to distinctive disease processes. The logic is straightforward: if an individual with ME/CFS experiences one symptom, they should be statistically more likely to experience other symptoms within the same cluster, suggesting common underlying disease processes.
To test this hypothesis, the researchers first conducted an extensive review of the existing scientific literature to identify symptom groupings that appeared to be associated with particular biological mechanisms. They then analysed symptom data from 748 individuals with ME/CFS to determine whether the observed symptom patterns matched these predictions.
Key findings
The data largely supported the hypothesis. Symptoms fell into four distinct, statistically significant clusters:
- The Brain cluster comprised neurocognitive (affecting mental processes) and sensory symptoms, including brain fog, sensory hypersensitivity, visual disturbances, sleep problems, and headaches, suggesting a pattern consistent with central nervous system dysfunction.
- The Immune cluster grouped symptoms associated with immune dysregulation and infection-related experiences, reflecting previous findings of altered immune function in ME/CFS.
- The Autonomic cluster contained symptoms associated with dysregulation of the autonomic nervous system, including cardiovascular, respiratory, and temperature-regulation disturbances, supporting the view that autonomic dysfunction is a core feature of the illness.
- The Gut cluster encompassed gastrointestinal symptoms and emerged as a distinct domain rather than simply forming part of the immune cluster.
These findings support the view that ME/CFS is not only a complex and heterogeneous disease but may also involve multiple underlying biological processes that give rise to different symptom profiles or phenotypes (presentations). Put another way, the fact that certain symptoms consistently predict the presence of others suggests that ME/CFS follows identifiable biological patterns rather than representing a vague or arbitrary collection of complaints.
This has potentially important implications for clinical trials. A treatment that appears ineffective when tested across a large, heterogeneous patient population may still prove beneficial for a specific subgroup of patients characterised by a particular symptom cluster.
Limitations
Several limitations should be considered when interpreting these findings.
First, the study relied on self-reported symptom data, which introduces the possibility of recall bias and variability in how individuals interpret and report symptoms. This is particularly relevant in conditions such as ME/CFS, where symptom severity and presentation can fluctuate over time.
Second, although the sample size was decent, participants were recruited through patient networks and support organisations. This may introduce selection bias, as a result, generalisability to all people with ME/CFS may be limited.
Third, the cross-sectional design captures symptom patterns at a single time point. This prevents assessment of how symptom clusters may evolve over time or whether they remain stable across different stages of illness.
Fourth, the analysis is based on statistical co-occurrence of symptoms rather than direct biological measures. Whilst the resulting clusters may reflect underlying physiological processes, this cannot be confirmed from the available data.
Further replication in independent cohorts and integration with objective biological markers will be important to establish the robustness and clinical relevance of these findings.
Conclusion
Ultimately, whilst the study does not prove the underlying mechanisms responsible for these patterns, it strengthens the case for viewing ME/CFS as a multisystem disease and may help guide future research towards more targeted approaches to diagnosis and treatment.