| NB: When considering information concerning groups of people with ME/CFS and those with long COVID, it is important to remember that ME/CFS is a symptom-based clinical diagnosis not a mechanistic one. It is clear there is a high degree of shared pathophysiology between ME/CFS and long COVID, and the two diagnostic labels are not mutually exclusive. Importantly, some individuals with long COVID meet ME/CFS diagnostic criteria or could have a dual diagnosis. |
Key points
- Although many studies on the prevalence of LC exist, there is not yet sufficient evidence to draw a conclusion about the proportion of people who go on to develop LC following a COVID-19 infection.
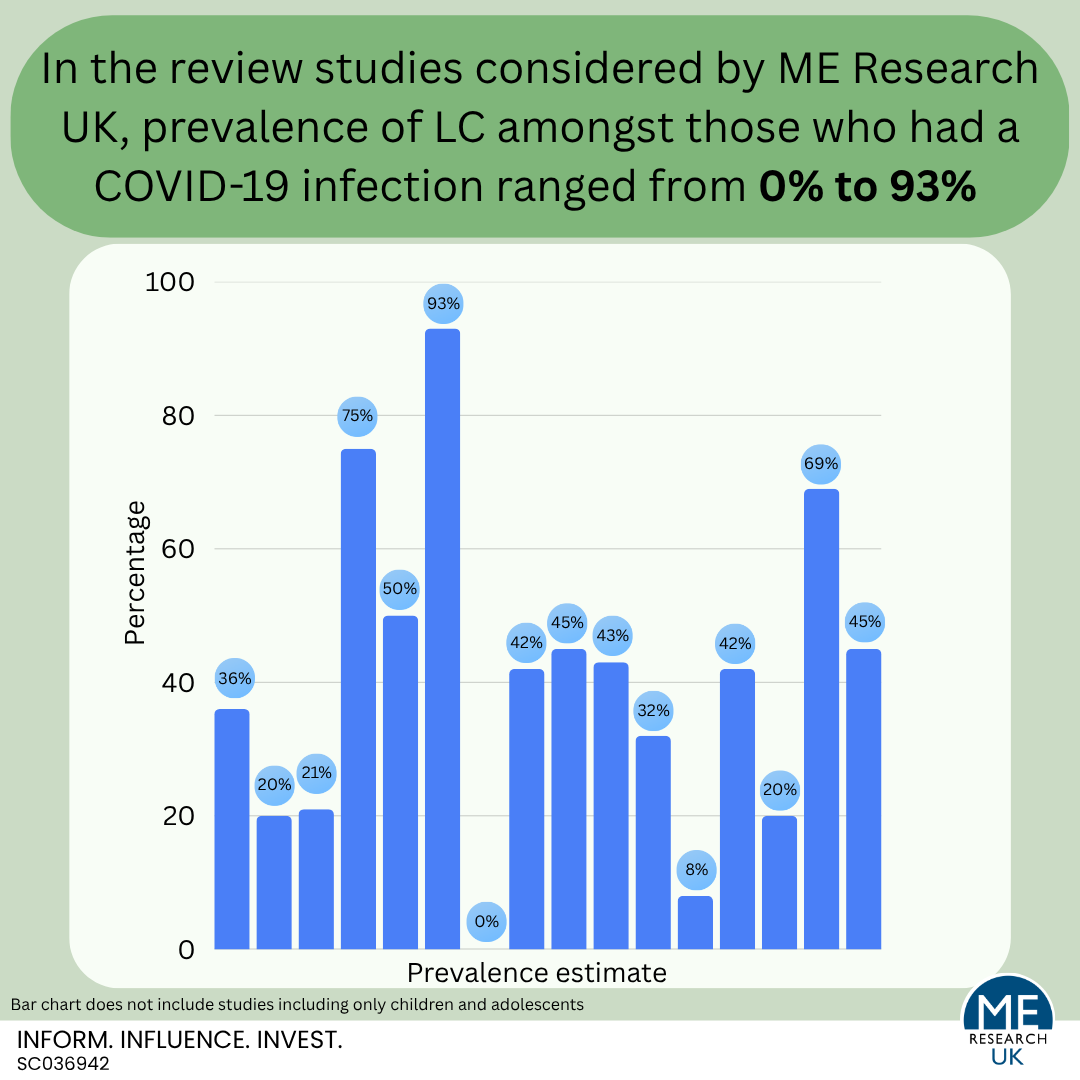
- Current evidence suggests that the prevalence of LC among those who had a COVID-19 infection ranges from 0% to 93%.
- While the true estimate will lie somewhere between the two, the extremes of no people (0%) and almost everyone (93%) are very unlikely.
- Studies comment on the high variation in estimates due to differences in factors including, but not limited to, sample populations, LC definitions, study design, and length of follow up.
Introduction
There are many studies which provide an estimate for the proportion of those who had a COVID-19 infection that go on to develop long COVID (LC). Rather than looking at all the available evidence (which would be a task for a research team with specialised skills in evidence synthesis, likely with the help of machine learning techniques) this section will consider the most recent systematic review evidence, alongside some noteworthy multinational studies.
The most recent review evidence
The most recent systematic review – a type of study that uses repeatable methods to search for, select, and combine all available evidence to answer a specific research question – comes from a study by Huo and colleagues published in 2025.
The review included a total of 429 studies (including over 2 million individuals) published between the 5th of May and 23rd of July 2024. Of these studies, 144 provided results which could be combined into a ‘pooled’ estimate; a figure derived by merging data from two or more samples, populations, or studies with the aim of producing a single, more precise estimate. Findings indicated that, globally, approximately 36% of people who had a COVID-19 infection went on to develop LC. Although prevalence differed significantly by geographical location, whether participants were hospitalised during the acute phase of COVID-19 infection (hospitalisation status), follow up time, biological sex, and age.
In their paper, the research team explain that their results may overestimate the proportion of people with LC because:
- Findings relate to lifetime prevalence of LC (i.e., ‘ever having long COVID’), and those who have now recovered, or who no longer meet diagnostic criteria for the illness, are included as cases.
- The LC definition used, ‘the presence of at least one new or persistent symptom at a follow up time of at least two months since a COVID-19 infection’, requires a shorter duration of symptoms compared with other, more widely recognised, criteria such as those from the NHS which state that LC occurs “when the symptoms of COVID-19 last longer than 12 weeks” and from the World Health Organisation (WHO) “continuation or development of new symptoms 3 months after the initial SARS-CoV-2 infection, with these symptoms lasting for at least 2 months with no other explanation“.
Also highlighted by the authors is the substantial variation (heterogeneity) in LC estimates across studies included in their review due to sources of what the team calls:
- ‘True heterogeneity’ – differences between study populations in factors such as age distribution, access to healthcare and healthcare quality, genetics, vaccine access and uptake, and prevalence of pre-existing comorbidities.
- ‘Study design and measurement induced heterogeneity’ – differences in the LC definition used, sampling selection, definition of subgroups within the population; for example, the definition of participants hospitalised during the acute phase of COVID-19 infection varied between studies.
Results from other international review evidence
The results from 21 studies included in this review indicated that approximately 20% of those who were hospitalised with an acute COVID-19 infection were still experiencing at least one persistent symptom three years after initial infection. Additionally, older age, higher COVID‐19 severity at hospitalisation, female sex, smoking, substance use, allergy, and having comorbidities (including congestive heart failure, chronic kidney disease, hypertension, and diabetes) were all associated with a higher risk of LC. As these results are from hospitalised patients only, the prevalence rate identified in this study is likely to be different to that of the general population. In fact, the authors state that “a key limitation of this review is the availability of data on persistent symptoms in hospitalized patients with little or no data regarding residual symptoms in patients with a mild course of COVID‐19“.
This umbrella review (a review of other review studies) included information from fourteen papers, and found that the prevalence of at least one LC symptom four weeks or more after SARS-CoV-2 infection ranged from 21% to 74.5%. Again, it is important to recognise that the definition of LC used by the researchers may overestimate prevalence.
Results also indicated that vaccination status, female sex, acute COVID-19 severity, and comorbidities were all associated with risk of LC. In this study, the authors considered LC as at-least one patient-reported, clinically presented, or administrative (e.g., ICD-10 codes) outcome associated with LC. In this paper, the researchers concluded “A high level of heterogeneity render the interpretation of pooled prevalence estimates of Long COVID challenging.”
This review aimed to look at changes in the prevalence of LC over one year and included 137 studies published between January 2020 and February 2022. Results suggested that 55% of people who had a COVID-19 infection experienced at least one LC symptom at one month follow-up, and that this rate decreased to approximately 50% by the 1-year follow-up. In this review, female sex, obesity, severe COVID-19 infection and hospitalisation status were all associated with an increased risk of developing LC. Again, the definition of LC used here may overestimate the prevalence, and the researchers highlight the “substantial heterogeneity in the results“.
This was a systematic review of 120 studies published between 1st January 2020 and 2nd November 2021. Studies were included if they reported, in English, the prevalence of LC, and included more than 100 participants – importantly, participants did not all need to be hospitalised in the acute phase of the illness.
For the purposes of Woodrow’s review, LC was defined as “persistent (constant, fluctuating or relapsing) symptoms and/or functional disability and/or the development of new pathology after SARS-CoV-2 infection for equal to or more than 12 weeks from onset of symptoms or from time of diagnosis, in people in whom the infection is self-described, clinically diagnosed, and/or diagnosed through a laboratory test”.
Results suggested that the prevalence of persistent symptoms in the included studies ranged from 0% to 93%, with a pooled estimate of 42.1%. It is also worth noting that the range in which the researchers could be certain that the true pooled estimate lies (the 95% prediction interval) was wide – between 6.8% and 87.9% – indicating high heterogeneity between studies. Based on their findings, the research team concluded that “the way in which LC is defined and measured affects prevalence estimation. Given the widespread nature of SARS-CoV-2 infection globally, the burden of chronic illness is likely to be substantial even using the most conservative estimates.”
O’Mahoney and colleagues (2023)
Using a statistical method – meta-analysis – that combines data from multiple independent studies to calculate a single, more precise, and reliable effect size, a systematic review of 194 studies (five of which were conducted in those less than 18 years of age), totalling 735,006 participants, found that “on average, 45% of COVID-19 survivors, regardless of hospitalisation status, were experiencing a range of unresolved symptoms at ∼ 4 months”. In this study LC was defined as “confirmed or self-reported COVID-19 symptoms at more than or equal to 28 days following infection onset“. Again, this definition may overestimate the number of people with LC compared to one which requires the presence of symptoms for over 12 weeks. As with other research teams, O’Mahoney and colleagues surmised that “current understanding is limited by heterogeneous study design, follow-up durations, and measurement methods”.
Another systematic review, which included 50 studies published between 5th July 2021 and 13th March 2022, reported that, based on a meta-analysis of 41 of the included studies, the prevalence of LC amongst those who had a COVID-19 infection was approximately 43%. Here, LC was defined as “having (1) any symptoms or (2) at least 1 new or persisting symptom during the follow-up time”.
In this study, the follow-up time was grouped into symptoms at 28–30 days, 60 days, 90 days, and 120 days. Notably, the team states that “although our post COVID-19 condition definition diverges from the WHO’s, we note that our estimates at 90 and 120 days may best reflect the current consensus definition” – this was 32%. Again, this study highlighted that there was substantial heterogeneity between study estimates, and that prevalence estimates differed by age, hospitalisation status, region and length of follow up.
This umbrella review of 23 review studies and the 102 primary studies within these published reviews identified that LC prevalence varied from 7.5% to 41% in samples of participants who were not hospitalised during the acute phase of their infection, and between 2.3% and 53% for samples combining both those who were hospitalised and those who were not. Again, the researchers commented on the heterogeneity of LC research stating “the heterogeneity and premature state of current research does not allow for confident statements on Long COVID’s prevalence, neither on its broader public health nor an economic burden”.
Notably, this review also identified three studies which estimated the prevalence of LC in children and teenagers; results from two studies suggested that LC prevalence in those who were not hospitalised ranged between 2% and 2.9%. One other study looked at a sample of both non-hospitalised and hospitalised children, reporting a prevalence of 3.5%. Here hospitalised children made up 3% of the sample. It is worth highlighting that these studies had small numbers of LC cases, or information was self-reported, or reported by a parent or carer if too young to self report. These limitations mean that the results should be interpreted with caution.
Overall, this study concluded that the “current evidence is still heterogeneous and incomplete“.
Pellegrino and colleagues (2022)
This review of 22 articles, published on or before the 15th of February 2022, looked specifically at the evidence relating to the prevalence of LC in children and adolescents. Results suggested that prevalence ranged from 1.6% to 70%, this may be partially explained by the variation in follow-up time after initial COVID infection, which varied between 4 weeks and 13 months. The study team also observed that older age, female sex and previous long-term health conditions were more frequently associated with LC. In the conclusion, the team emphasised that “evidence on long COVID in children is limited, heterogeneous, and based on low-quality studies“.
Non-review evidence worth considering
Although not a review study, another paper worth noting is this online, multinational survey carried out between April 2022 and January 2023. Respondents were 11,801 people from 33 different countries aged 18 years or older with a previously confirmed COVID-19 infection. LC was defined, in line with the WHO definition, as “Development of signs and symptoms during or after an infection consistent with findings typical of COVID19 that continue for more than 12 weeks and cannot be matched to an alternative diagnosis.” Results showed that 19.8% of survey respondents with PCR-confirmed COVID-19 had self-reported LC and 80.2% did not. Interestingly, this study also identified factors associated with an increased risk of LC, including ICU admission, female sex, and acute fatigue, and those linked with a decreased risk such as African American and Asian ethnicities, and receiving even one dose of COVID-19 vaccination.
Pazukhina and colleagues (2024)
Also worth considering is a study of 11,860 adult participants from 17 different countries who had been hospitalised with a confirmed COVID-19 infection between February 2020 and April 2022. Countries of origin were classed as high income countries (HICs: France, Gibraltar, Israel, Italy, Norway, Portugal, Spain and the UK) or lower and middle income countries (LMICs: Brazil, Colombia, The Gambia, India, Malaysia, Russian Federation, South Africa, Sudan and Ukraine).
The participants were followed up, and the prevalence of persistent symptoms assessed at 2 timepoints: between 2 months and anytime up to (but not including) 6 months post-hospital discharge, and between 6 months and anytime up to 12 months post-hospital discharge. Importantly, those with at least one persistent symptom, not present prior to the onset of COVID-19, at the first follow-up assessment were categorised as having LC.
Results indicated that LC affects populations across the globe, with similar symptoms and impact on functioning in both HICs and LMICs. However, the proportion of hospitalised participants who went on to report ongoing symptoms was significantly higher in HICs compared with LMICs (69.0% versus 45.3%), something the research team state “may reflect better awareness, along with a broader range of reported symptoms, including significant neurocognitive and psychosocial issues” in HICs and possible “under-reporting due to limited healthcare access and resources” in LMICs.
Summary
Current evidence suggests that the prevalence of LC among those who had a COVID-19 infection ranges from 0% to 93%. The true figure will lie somewhere between these two unlikely extremes.
All review studies comment on the high variation in estimates due to differences in factors including, but not limited to, sample populations, LC definitions, study design, and length of follow up.
The main conclusion that can be drawn here is that although many studies on the prevalence of LC exist, there is not yet sufficient evidence to draw a conclusion about the proportion of people who go on to develop LC following a COVID-19 infection.