Key points
- There are many difficulties faced when attempting to estimate the prevalence of LC. In this, the second of two articles, ME Research UK highlights the following issues:
- How awareness of LC, medical gaslighting, and avoidance of diagnosis due to stigma might influence prevalence estimates.
- The complexity and number of risk factors which impact the LC prevalence.
- The heterogeneity of LC.
- While estimates of the prevalence of LC exist, they are limited by a number of factors such as the definition used, how representative the study population is of the general population, and how reliable the methods are.
- Estimates change over time, and vary between countries (and between different research studies), meaning that it is not always appropriate to directly compare estimates or to extrapolate figures to populations for which they were not intended/beyond that for which they were initially calculated.
Introduction
In this, the second of two articles discussing the difficulties faced when attempting to reach a consensus regarding a prevalence estimate for long COVID (LC), ME Research UK will highlight:
- How awareness of LC, medical gaslighting, and avoidance of diagnosis due to stigma might influence prevalence estimates.
- The complexity and number of risk factors which impact the LC prevalence.
- The heterogeneity of LC.
Awareness of LC, medical gaslighting, and avoidance of diagnosis due to stigma
In the “long COVID status report”, which was published in February 2025 to summarise evidence relating to LC, authors highlight issues relating to medical gaslighting. In the report, the authors explain that “many patients have gone undiagnosed, faced scepticism, received inadequate evaluations, or been given inappropriate treatments”. This may mean that some people with LC are not told they have the illness by a medical professional, or they may be misdiagnosed with another condition like anxiety or depression – regrettably, both misdiagnosis and medical gaslighting are frequently experienced by those with ME/CFS, including a proportion of those with LC who meet ME/CFS diagnostic criteria.
Additionally, some people may experience more barriers to seeking help from health care professionals for LC than others. For example, a paper published in the British Journal of General Practice in 2024 identified that people from ethnic minority groups reported that “experiences of stigma and discrimination contributed to delays in seeking care and unsatisfactory experiences, resulting in feelings of mistrust in health care“. This could mean that prevalence rates may appear artificially low in these groups, especially where estimations are based on data from medical records.
Another paper, published in 2026, notes that where studies ask participants whether or not they have LC, their answer is dependent on them knowing what LC is.
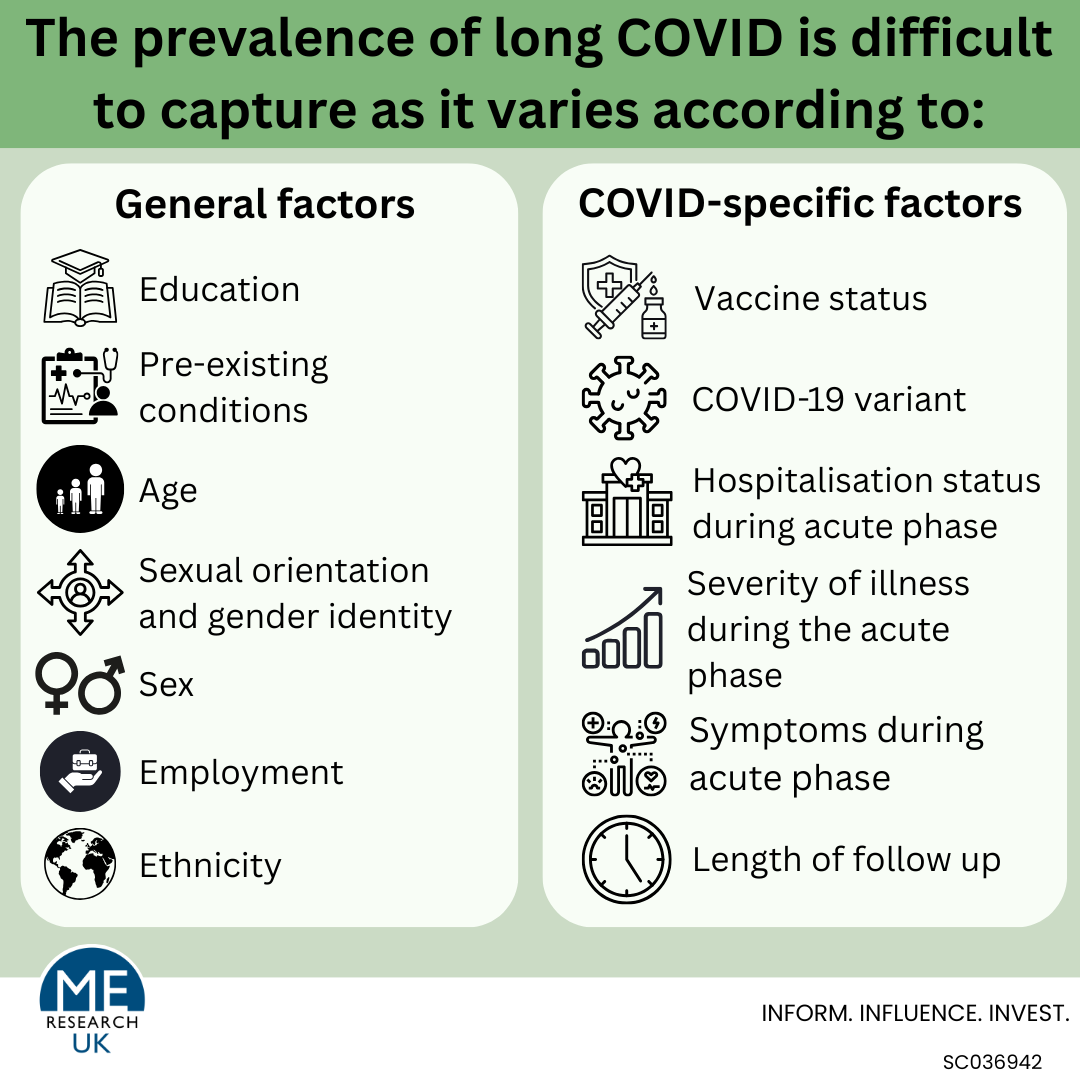
Complexity and number of LC risk factors
Research suggests that the prevalence of LC is impacted by a number of different factors; these include COVID-related factors and more general characteristics. These factors are especially important to consider when comparing or combining results from different studies. Where studies have used different sample populations, prevalence could vary widely based on not only the age, sex, and ethnic make-up of the population, but also the proportion of people who had the Omicrom COVID variant, the number who were unvaccinated, and how many were hospitalised. Often, some of this information (especially that relating to COVID variant and reinfection status) has not been collected making it extremely hard for researchers to take these factors into account in the analysis.
Examples of COVID-related factors:
- Symptoms experienced during the acute phase of COVID infection – one study found that those who experienced fatigue during the acute phase of infection were more likely to develop LC.
- Severity during the acute phase of illness – There is conflicting evidence to say whether more, or less severe COVID infections lead to a higher risk of LC. One study, which considered the prevalence of LC across 33 countries, identified a higher prevalence of LC among those who had been admitted to an intensive care unit during the acute illness phase. While this has not been consistently observed in all prevalence studies, with some suggesting that less severe COVID-19 infection is linked with an increased risk of LC, it is worth noting that in some instances, potential cases of LC may have been lost amongst those who had severe COVID-19, but sadly did not survive.
- COVID-19 variant – Some studies have suggested that LC prevalence may vary depending on the COVID variant (such as Omicron, Alpha, and Delta). One study found that a disproportionately large percentage of patients who first tested positive for COVID-19 while the wild-type, Alpha, and Delta variants were dominant went on to develop LC. Conversely, a disproportionately small share of those who first tested positive for COVID-19 while the Omicron variant was most prevalent went on to develop LC.
- Reinfection – Some research has indicated that LC prevalence may be different for those who only had one COVID-19 infection, compared with those who have had more than one infection.
- Vaccine status – there is mixed evidence relating to vaccine status and LC prevalence; some studies suggest that rates of LC are lower in populations who have had the vaccine.
Examples of general factors:
- Sex: Across multiple studies, LC prevalence has been found to be higher in females than males. While there is evidence to suggest that differences in the immune system between males and females may lead to sex differences in the risk of developing post-acute infectious syndromes, including LC, it is important to note that men may also be less likely to report symptoms due to the stigma associated with fatigue-related illnesses, something identified among men with ME/CFS.
- Age: In some studies, older age was associated with a higher risk of LC. However, in others age was not found to be associated with the number of people who develop ongoing symptoms following a COVID-19 infection – it is worth noting that this study only included a small number of participants. The significance of the association may also depend on how age was looked at – whether it was each yearly increase in age, or one age group compared with another. There has also been research looking specifically at the prevalence of LC in children and young people, which found that even within those aged 11–17 years, prevalence was varied, with LC more common amongst those aged 15–17.
- Ethnicity: Prevalence of LC has been found to vary by ethnic group; for example, one study found that ‘some people of colour’ were more likely to have, and to experience activity limitations from, LC.
- Sexual orientation and gender identity – Those in sexual and gender minority groups have been found to have higher prevalence of LC.
- Education – Research has found that those with a graduate education compared with high school or less are less likely to experience “persistence of LC”.
- Employment – Workers in jobs associated with a higher risk of catching COVID-19, such as health and social care, education, retail, transport and security have been found to have a higher LC risk.
- Urban vs rural location – Those in urban locations have been found to be less likely to have ongoing LC symptoms compared with those who live in rural areas.
- Pre-existing conditions – Research has suggested that people with pre-existing conditions – such as obesity and asthma – are more likely to develop LC, meaning that there is a higher prevalence of the disease in these groups.
It is worth noting that many studies investigating LC risk factors were limited by small sample sizes, especially within subgroups of the population; for example, for ethic minority groups, which limits the conclusions that can be drawn.
LC disease heterogeneity
The 2022 NICE guidance on LC states that the “The signs and symptoms after acute COVID-19 are highly variable and wide-ranging, and may fluctuate, with exacerbations triggered by physical or mental stress.” This means that the symptoms of LC can vary widely among those with the illness, making identification of ‘cases’ for prevalence calculations more complex.
In fact one US study, which followed up 3,659 participants with a history of SARS-CoV-2 infection from the RECOVER-Adult Cohort Observational Study over 15 months, identified eight distinct patterns of symptom burden, which the researchers called ‘profiles’:
| Description | % of the population |
| “Persistent, high symptom burden” | 5 |
| “Intermittently high symptom burden” | 12 |
| “Improving, moderate symptom burden” | 10 |
| “Improving, low symptom burden” | 9 |
| “Worsening, moderate symptom burden” | 8 |
| “Delayed worsening symptom burden” | 6 |
| “Consistent, low symptom burden” | 13 |
| “Consistent, minimal to no symptom burden” Note – This group described “participants who never met the threshold for Long COVID” | 36 |
Although more research would be needed in different groups of participants to establish whether these profiles can be seen in other populations with LC, the findings from this study highlight disease heterogeneity. In an illness that has no validated diagnostic biomarker, this heterogeneity could complicate the diagnostic process, increasing the risk of mis-diagnosis which in turn impacts the accuracy of prevalence rates.
Summary
In part 1 of this article, ME Research UK highlighted how methodological differences – such as use of different study designs, variations in how LC is defined, and issues with accurate identification of LC cases now COVID-19 testing is no longer routine – can impact prevalence estimates. In this, part 2 of the discussion around the difficulties in arriving at a consensus regarding the prevalence of long COVID, issues relating to awareness, medical gaslighting, and stigma have been highlighted, alongside how the complexity and number of risk factors for LC, and the heterogeneity of the disease itself, also impact the prevalence.
In conclusion, without a validated diagnostic biomarker, accurately capturing LC prevalence will remain an ongoing challenge for researchers, especially in the absence of routine testing for COVID-19.
What does the evidence tell us about the prevalence of long COVID?