| NB: When considering information concerning groups of people with ME/CFS and those with long COVID, it is important to remember that ME/CFS is a symptom-based clinical diagnosis not a mechanistic one. It is clear there is a high degree of shared pathophysiology between ME/CFS and long COVID, and the two diagnostic labels are not mutually exclusive. Importantly, some individuals with long COVID meet ME/CFS diagnostic criteria or could have a dual diagnosis. |
Key points
- It is still unclear exactly what proportion of those with LC meet ME/CFS diagnostic criteria.
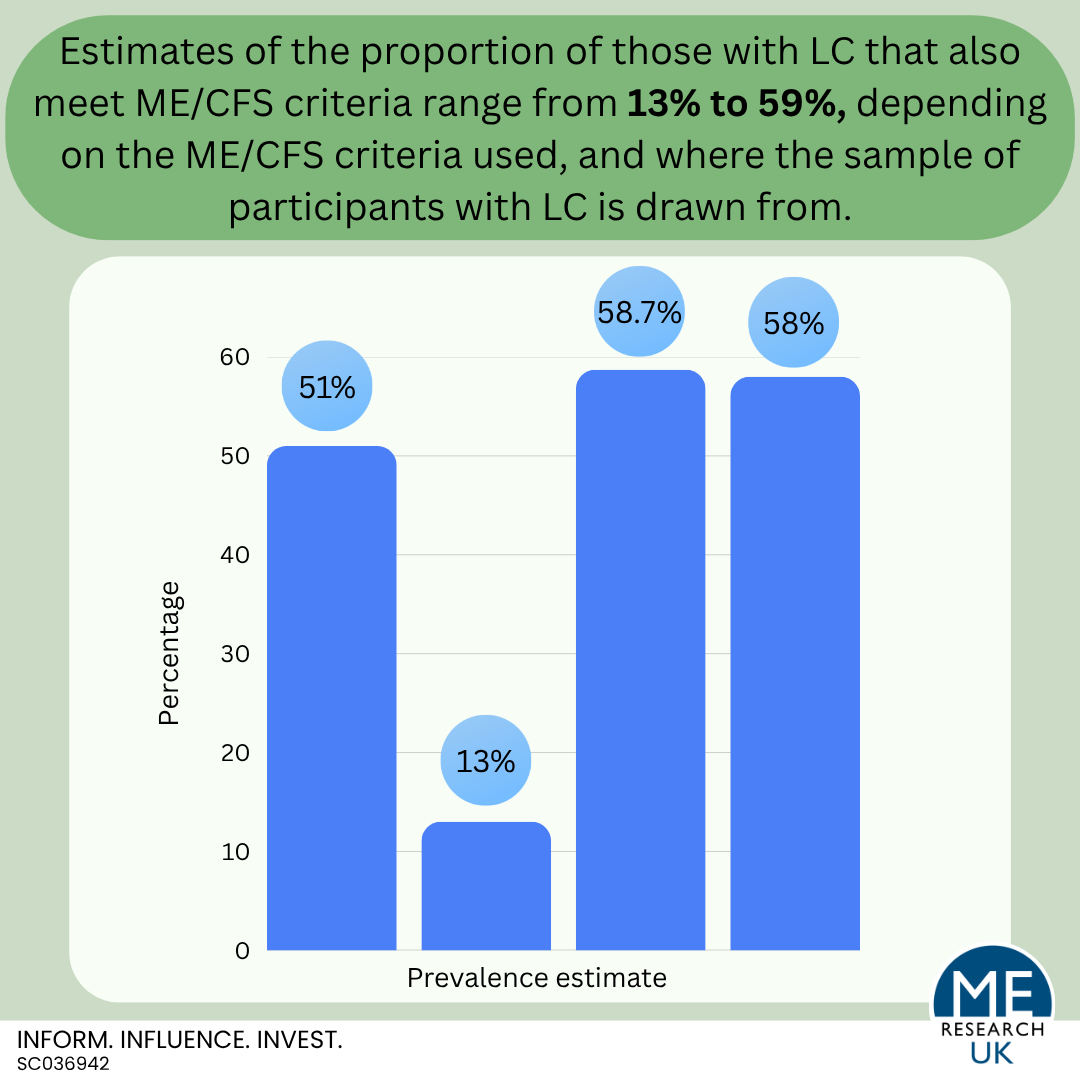
- Although recent estimates vary widely (between 13 and 59%), rates vary depending on the ME/CFS criteria used, and where the sample of participants with LC is drawn from.
Introduction
The overlap in symptoms between LC and ME/CFS means that some people with LC also meet diagnostic criteria for ME/CFS, although the exact proportion varies depending on the ME/CFS criteria used. Importantly, SARS-CoV-2 infection is associated with the onset of ME/CFS symptoms in some individuals (as for some individuals their long COVID presentation was purely ME/CFS).
The most recent systematic review evidence
A systematic review of 13 studies published between January 2020 and May 2023 concluded that 51% of 1,973 people with LC met ME/CFS diagnostic criteria requiring PEM for a diagnosis to be made (the Canadian Consensus Criteria (CCC), International Consensus Criteria (ICC), Institute of Medicine (IOM), and the DSQ). The authors suggest that those with LC meeting ME/CFS criteria may represent the more severe cases of LC. It is important to note that the participants with LC were identified using one of nine different standardised questionnaires, this may have led to higher heterogeneity among people with LC than would have been present had only one standardised questionnaire been used. It is possible the variety of LC questionnaires used may have impacted the findings observed. Additionally, in a letter to the editor of the Journal of Infection, former ME Research UK-funded researchers Dr Nuno Sepúlveda and Dr Francisco Westemeier highlighted several potential methodological issues with the review by Dehlia and Guthridge that may mean that the main finding – that approximately 50% of people with LC meet ME/CFS criteria – is likely to be an overestimation that can be explained by “biased samples” recruited from LC support groups rather than from the general population.
Non-systematic review evidence worth considering
Although included as one of the 13 studies in the above systematic review, this study by Prof. Leonard Jason is worth considering in more detail as it focuses on the limitations of existing evidence.
Jason’s work, published in December 2022, noted that, at time of publication, existing estimates for the proportion of people with LC who meet ME/CFS criteria ranged from 13% to 58.7%. However, the studies providing these estimates were limited by factors such as small sample size, “unclear methods for determining the ME/CFS case definitions”, and a lack of comprehensive measures for post-exertional malaise (PEM).
Therefore, Jason’s 2022 study aimed to overcome some of the methodological limitations by using a short-form version of the De Paul Symptom Questionnaire as a standardised method to identify ME/CFS. Based on this, approximately 58% of participants with LC met ME/CFS criteria.
However, this study had its own limitations which limit the conclusions that can be drawn:
- A higher female/male ratio than most other studies.
- Lack of ethnic diversity.
- “Study subjects were recruited from online patient communities of people whose COVID-19 was diagnosed in various ways.”
- A cross-sectional study design was used which only provides a snapshot in time. Long-term follow-up would be needed to determine if ME/CFS symptoms persist in the sample population.
Grabowska and colleagues (2023)
This opinion article, by a team of researchers including current and former ME Research UK-funded scientists Dr Nuno Sepúlveda, Dr Francisco Westemeier and Dr Eliana Lacerda, stated that despite widespread awareness of the similarities between LC and ME/CFS, many LC studies had missed the opportunity to fully assess the presence and severity of key features of ME/CFS, including PEM. Regrettably, this means that there is minimal evidence accurately assessing the proportion of people with LC who meet ME/CFS criteria, and the evidence that does exist has many limitations.
In their article, the researchers recommended that future epidemiological studies assessing the prevalence of LC should also incorporate standard questionnaires for ME/CFS diagnosis such as the DSQ or UK ME/CFS Biobank (UKMEB) diagnosis Symptoms Assessment Questionnaire, and those assessing ME/CFS symptoms such as the DSQ-PEM. Importantly, the team highlight that this can be done at minimal cost. Additionally, they recommend reporting as standard:
- ME/CFS case definition used,
- Symptom inventory,
- Excluded medical and psychiatric conditions and co-morbidities,
- Self-reported functional impairment/levels of activity.
The team state that having this information accurately recorded would better enable comparisons between studies and the pooling of study estimates, both of which are required to reach a consensus about the proportion of people with LC who meet ME/CFS critera.
Summary
It is still unclear exactly what proportion of those with LC meet ME/CFS diagnostic criteria. Although recent estimates suggest between 13 and 59%, rates vary depending on the ME/CFS criteria used, and where the sample of participants with LC is drawn from.
In the future, research should use:
- ME/CFS criteria that requires PEM for a diagnosis to be made.
- Participants from the general population rather than predominantly those who attended an LC clinic, or only those who developed LC after hospitalisation in the acute phase of the disease.
- Methods which follow participants up over time (longitudinal research).