| NB: When considering information concerning groups of people with ME/CFS and those with long COVID, it is important to remember that ME/CFS is a symptom-based clinical diagnosis not a mechanistic one. It is clear there is a high degree of shared pathophysiology between ME/CFS and long COVID, and the two diagnostic labels are not mutually exclusive. Importantly, some individuals with long COVID meet ME/CFS diagnostic criteria or could have a dual diagnosis. |
Key points
- Prevalence is the percentage (or proportion) of the population that has a certain characteristic or is affected by a particular disease; here we are considering those with Long COVID (LC).
- LC is an umbrella term encompassing all conditions and prolonged symptoms following/associated with a SARS-CoV-2 infection.
- Importantly, some individuals with LC meet ME/CFS diagnostic criteria or have a dual diagnosis.
- Knowing the proportion of people who have LC is important for several reasons including estimation of the proportion of people who have a disease in a population at a given time, identification of groups of the population who may be more at risk of a disease by looking at prevalence by factors such as age, ethnicity, or sex, and for allocating health resources or justifying the importance of research.
- For both LC and ME/CFS, accurately estimating prevalence is extremely difficult.
- While, ME Research UK has previously discussed the challenges associated with ME/CFS prevalence, this series of articles will take a closer, unbiased look at the prevalence of LC.
What is long COVID?
Long COVID (LC) is an umbrella term encompassing all conditions and prolonged symptoms following/associated with a SARS-CoV-2 infection.
The National Academies of Sciences, Engineering, and Medicine (NASEM) define LC as:
“An infection-associated chronic condition that occurs after SARS-CoV-2 infection and is present for at least three months as a continuous, relapsing and remitting, or progressive disease state that affects one or more organ systems.”
Last revised in October 2022, the NICE guidance on LC states:
“The signs and symptoms after acute COVID-19 are highly variable and wide-ranging, and may fluctuate, with exacerbations triggered by physical or mental stress.”
Further information provided by NICE details that:
- “Some people experience multi-organ effects or autoimmune conditions,
- There may be evolution of symptoms including permanence of symptoms, and the development of new symptoms or conditions,
- There may be a worsening of pre-existing symptoms or conditions.“
Importantly, people with LC have a wide range of symptoms, meaning the illness is “heterogeneous“, or that it varies widely between person to person.
NICE states that the most commonly reported symptoms include (but are not limited to):
- Generalised symptoms: fatigue, fever, and pain, and for some post exertional malaise (PEM).
- Cardiovascular symptoms: chest pain, chest tightness, and palpitations.
- Dermatological symptoms: skin rashes and hair loss.
- Ear, nose and throat symptoms: Dizziness, earache, loss of taste and/or smell, nasal congestion, sore throat, and tinnitus.
- Gastrointestinal symptoms: Abdominal pain, diarrhoea, nausea and vomiting, weight loss and reduced appetite.
- Musculoskeletal symptoms: Joint and/or muscle pain.
- Neurological symptoms: Autonomic dysfunction, cognitive impairment, headaches, mobility impairment, sleep disturbance, and visual disturbance.
- Respiratory symptoms: Breathlessness, and cough.
- Psychological symptoms: Anxiety, depression, and post traumatic stress disorder (PTSD).
It can be observed that some of the symptoms of LC – such as PEM, pain, cognitive impairment, and fatigue – overlap with ME/CFS, and COVID-19. ME/CFS is a specific clinical diagnosis requiring the presence of core symptoms for a specific time period. This means that some people with LC also meet the diagnostic criteria for ME/CFS, although the exact proportion depends on the ME/CFS criteria used such as the NICE 2021 guideline, the Canadian Consensus Criteria (CCC) or the Institute of Medicine (IOM) Criteria.
What is prevalence?
Prevalence is the percentage (or proportion) of the population that has a certain characteristic or is affected by a particular disease; here we are considering those with LC.
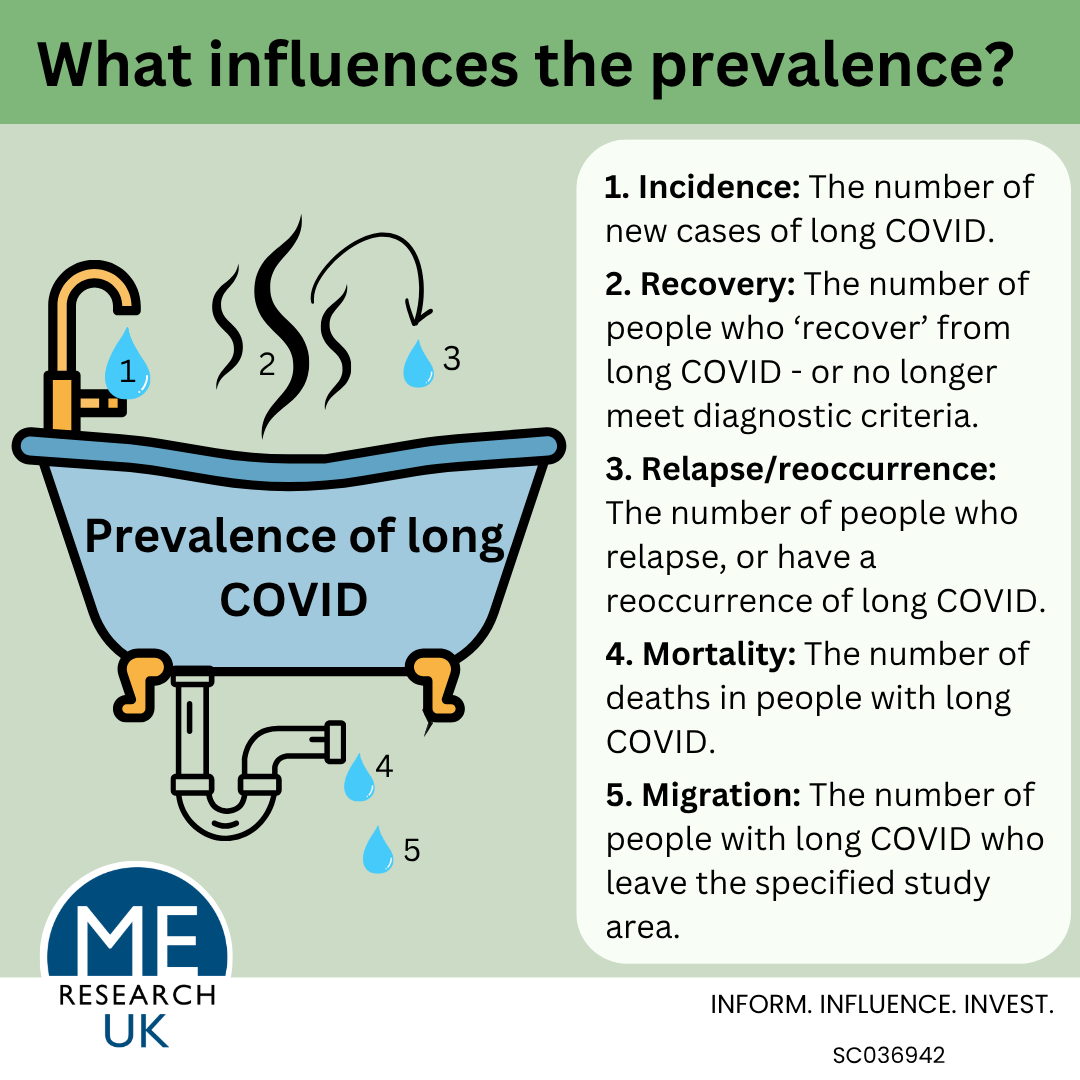
Independent of the disease of interest, several different factors can influence prevalence. These are:
- Incidence: the number of new cases of the disease.
- Recovery: the number of people who recover from the disease – or who no longer fulfil diagnostic criteria.
- Relapse/reoccurrence: the number of people who have a relapse or reoccurrence of the disease.
- Mortality: the number of deaths in people with the disease.
- Migration: the number of people with the disease who move out of the study area.
Different types of prevalence estimate
The main types of prevalence used in epidemiology – the study of diseases in populations – differ based on the window of time being assessed, and include the proportion of a population with a condition at a specific single point in time (point prevalence), the proportion of individuals who have ever experienced a condition or disease (lifetime prevalence), and the proportion of a population with a condition at any point during a defined period, such as a month, a year, or several years (period prevalence).
Why are prevalence estimates used?
Generally, prevalence figures are useful for several reasons:
- To provide an estimate of the proportion of people who have a disease in a population at a given time (or over a specified time period).
- To identify groups of the population who may be more at risk of a disease by looking at prevalence by factors such as age, ethnicity, or sex.
- It can be used – alongside the impact of a specific disease on an individual and wider society – when:
- Allocating health care resources;
- Justifying the importance of research;
- Applying for/allocating research funding;
- Helping to raise awareness of the impact of a disease.
- To provide an indication of the economic burden – the cost – of a disease.
Why do prevalence estimates differ?
The choice of which prevalence estimate is used is not wholly a research matter – the choice can be dependent on the purpose for which the estimate will be used. For example, an estimate used to raise awareness of a disease may use research findings which legitimately report a higher prevalence figure and choose to ignore a lower reported figure.
Likewise, different types of prevalence estimate are used for different reasons. For example, point prevalence, which provides a snapshot in time, is used for acute, fast-moving outbreaks like the flu, whereas period prevalence, which details cases over a specific duration, is better for chronic diseases like diabetes, that last a long time.
Different types of estimate can lead to larger or smaller values for the prevalence of the same disease due to differences in methods and the data used to calculate them.
Here it is worth considering lifetime prevalence which estimates the proportion of people who have had the illness of interest at any point in their lives up to the time of measurement, in comparison with period prevalence which measures the proportion of a population with a condition over a specific period of time.
Importantly, not only do the methods used to calculate these estimates vary, but so do the limitations:
- Period prevalence is often based on data which does not include individuals with mild, undiagnosed, or asymptomatic cases, leading to potential underestimation of prevalence.
- For lifetime prevalence, researchers are unable to distinguish between active and past cases (i.e. whether every person who is counted as a ‘case’ still has the disease), and this may mean that disease burden is over-estimated.
Why is a prevalence figure for long COVID so important?
Knowing the proportion of people who have LC is not only important for the reasons given above, but also because the prevalence of LC is closely tied to that of ME/CFS; SARS-CoV-2 infection can be associated with ME/CFS onset and, unsurprisingly, there is an overlap in symptoms between the two diagnoses.
Regrettably, estimates for ME/CFS are limited for a number of reasons, including that the proportion of people with LC who also meet ME/CFS diagnostic criteria is unknown. Knowing both the number of people who have LC, and the number of these who meet ME/CFS criteria (including those who have both LC and ME/CFS) is essential to ensure adequate care provision, and to calculate a more accurate number of people who have ME/CFS.
For both LC and ME/CFS, accurately estimating prevalence is extremely difficult. While ME Research UK has previously discussed the challenges associated with ME/CFS prevalence, this series of articles will take a closer, unbiased look at:
- What are the difficulties in arriving at a consensus regarding the prevalence of long COVID? – Part 1
- What are the difficulties in arriving at a consensus regarding the prevalence of long COVID? – Part 2
- What the existing research says about the prevalence of LC, alongside the research’s strengths and limitations.
- A summary, and recommendations for the next steps.