
Key points
- Both children and young people, under the age of 18 years old, can develop ME/CFS.
- The debilitating symptoms of ME/CFS on children and young people can have a huge impact on day-to-day family life, and a detrimental effect on the experiences of a child at school and on extra-curricular activities.
- The proportion of children and young people who have ME/CFS remains unclear.
- More research is needed to better understand the number of people under the age of 18 years living with the disease in different countries.
- As in the adult population, there is no single test that can be used to diagnose ME/CFS in children and young people.
- Diagnosis is based on the presence of key symptoms, medical history, and the exclusion of other medical conditions that may cause similar symptoms using different medical tests.
- Research recommends that parent/caregiver report(s) and self-report of the child or young person should both be obtained to provide “a more complete understanding” of the child’s health.
- More research is needed to understand ME/CFS in children and young people particularly that which aims to improve diagnostic procedures, health care, and access to education, and that which considers the impact of puberty on the risk – and symptom profile, of the disease.
ME/CFS in children and young people
Both children and young people, under the age of 18 years old, can develop ME/CFS.
Although the disease is more common in adolescents – those who are in the phase between childhood and adulthood (adolescence); defined by the World Health Organisation as those aged between 10-19 years old – than young children, ME/CFS has been reported in children aged just 2 years old.
A paper relating to the diagnosis and management of ME/CFS in young people stated that symptoms of the disease can vary from day to day, and even fluctuate within the same day.
Generally:
- Young people with mild ME/CFS “may be able to attend school full-time or part-time, but they might have to limit sport and after-school activities and have frequent school absences”.
- Those with more severe ME/CFS “can be wheelchair dependent, housebound, or bedbound. The more impaired might even have difficulty participating in home tutoring sessions”
While few studies have investigated ME/CFS in those under the age of 18 years – meaning that little is known about the disease in this age group, it is clear that the debilitating symptoms of ME/CFS can have a huge impact on day-to-day family life, and a detrimental effect on the experiences of a child at school and on extra-curricular activities.
Research suggests that ME/CFS is one of the leading causes of long-term medical leave from school, and a project funded by ME Research UK identified that the quality of life of children with ME/CFS was significantly reduced compared with their healthy counterparts.
How many children and young people have ME/CFS?
Currently, the proportion of people (prevalence) with ME/CFS is unclear – this is true both for adults, and for children and young people with the disease. This uncertainty is due to the lack of large-scale prevalence studies, differences in diagnostic criteria, delays in ME/CFS diagnosis, and misdiagnosis.
While estimates for the number of children and adolescents with ME/CFS do exist – ranging from almost 0% to as high as 3%, Professor Leonard Jason and colleagues have suggested that the studies used to acquire these figures are limited by:
- The methods used to diagnose ME/CFS – for example, the lack of medical examination.
- Use of study samples that do not accurately reflect diversity within the population.
In a study published in 2020, Professor Jason and his team aimed to address some of these limitations by recruiting a diverse group of 10,119 children and young people aged 5 to 17 years in the “Chicagoland area”, USA. In the study, ME/CFS was diagnosed by a medical doctor when a participant met three criteria; the Fukuda criteria with revisions recommended by Reeves and colleagues in 2003 (not specific to children and adolescents); the pediatric version of the DePaul Symptom Questionnaire, and the Institute of Medicine (IoM) criteria.
Findings showed that in this population, the prevalence of ME/CFS in the young was 0.75% or 750 in 100,000. Results also indicated that the prevalence of ME/CFS was higher among females than males – something also observed in adults with ME/CFS, and in “African American”, and “Latinx” children and adolescents compared with “Caucasian” children and adolescents. There were also differences in prevalence by age; those aged 12-14, and 15-17 had higher rates of ME/CFS than children aged 5-8, and 9-11 as shown in the table below:
| Prevalence rate | |
| Gender | |
| Female | 0.94% |
| Male | 0.58% |
| Race/Ethnicity | |
| Caucasian | 0.63% |
| African American | 1.11% |
| Latinx | 1.28% |
| Age (years) | |
| 5-8 | 0.14% |
| 9-11 | 0.45% |
| 12-14 | 0.82% |
| 15-17 | 1.25% |
The terms used in this table reflect those used in the original research paper.
It is important to note that while the study by Professor Jason does provide an estimate of ME/CFS prevalence in a diverse group of children and young people in the “Chicagoland area”, USA, this estimate may not be applicable to other areas of the USA, or other countries that have different population characteristics.
Other estimates for the prevalence of ME/CFS in children and young people in the USA include that from the CDC which suggests that “up to 2 in 1000 children” (0.2%) may have ME/CFS – although it is unclear where this estimate came from. Here, while no clear estimate is provided for the prevalence of ME/CFS in adolescents, the CDC does state that “ME/CFS is more common in adolescents than in younger children” – this is in agreement with the research from Professor Jason and colleagues.
Outside the USA, no recently published studies have estimated the number of children with ME/CFS. In the UK, a paper from 2003 suggested that when using the Fukuda criteria for CFS, the prevalence among 5-15 years olds studied was approximately 0.19%; in this study, chronic fatigue was defined as “severe fatigue of at least six months’ duration, for which rest did not help and which led to functional impairment of the child”. Another study from the UK – published in 2007, identified the prevalence of self-reported ME/CFS amongst 16-year-olds to be 1.9%.
Overall, it is clear that the prevalence of ME/CFS amongst children and young people remains uncertain, and more research is needed to better understand the numbers of people under the age of 18 years living with the disease in different countries. It is also important to establish whether the prevalence of ME/CFS differs in the various population groups within these countries (for example by ethnic group, in males and females, or pre-and post-puberty). Additionally, due to the overlap in symptoms between long COVID and ME/CFS, more research is needed to understand the impact of the COVID-19 pandemic and long COVID on the prevalence of ME/CFS in children and adolescents – as is the case for adults.
How is ME/CFS diagnosed in children and young adults?
As in the adult population, there is no single test that can be used to diagnose ME/CFS in children and young people. Therefore, diagnosis is based on the presence of key symptoms, medical history, and the exclusion of other medical conditions that may cause similar symptoms using different medical tests.
Several diagnostic criteria exist for diagnosing ME/CFS both in adults, and in children and young people. Regrettably, these criteria differ slightly, and criteria for children and young people diagnose both “ME” – The International Consensus Criteria (ICC) (2011), and “ME/CFS” – the NICE guidelines (2021) and the ME/CFS Pediatric Case Definition (2008). Additionally, the IoM diagnostic criteria diagnose ME/CFS but at the time of publication, this guideline recommended a new term for the illness “systemic exertion intolerance disease (SEID)” (2015). The IoM guidelines are now summarised on the CDC website – webpage last updated in April 2021, where the term ME/CFS is used.
Key differences between the criteria include the exact ME/CFS symptoms required, and the length of time these symptoms need to be present for a diagnosis to be made. The requirements for a diagnosis under the different criteria for diagnosing paediatric ME/CFS are summarised below.
| NICE 2021 ME/CFS criteria | |
| Requirements for a diagnosis | Exclusionary conditions: |
| To suspect ME/CFS: All of the following symptoms have been present for a minimum of 4 weeks: Debilitating fatigue Post exertional Malaise Unrefreshing sleep Cognitive difficulties (or ‘Brain fog’) Pre-illness activity levels should also have been significantly reduced. To make a diagnosis of ME/CFS: Diagnose ME/CFS in a child, young person or adult who has the symptoms above that have persisted for 3 months and are not explained by another condition. | Symptoms must not be explained by another condition – the guidelines give a list of medical tests that should be carried out to exclude other diagnosis |
| ME/CFS pediatric case definition (Jason et al 2008) | |
| Requirements for a diagnosis | Exclusionary conditions: |
| Critical symptoms for diagnosis: Post exertional malaise (PEM) and/or post-exertional fatigue Unrefreshing sleep or disturbance of sleep quantity or rhythm disturbancePain (or discomfort) “To be diagnosed with pediatric ME/CFS, the child or adolescent must have clinically evaluated, unexplained, persistent or relapsing chronic fatigue over the past 3 months that is not the result of ongoing exertion; is not substantially alleviated by rest; results in substantial reduction in previous levels of educational, social and personal activities; and must persist or reoccur for at least three months.” | Any active medical condition that may explain the presence of chronic fatigue with examples including multiple sclerosis, Lyme disease, and Lupus erythematosus. This criteria also lists “non-exclusionary disorders” These include co-occurring disorders that do not adequately explain fatigue such as anxiety disorders, and fibromyalgia. |
| The International Consensus Criteria (ICC) for ME (2011) | |
| Requirements for a diagnosis | Exclusionary conditions: |
| To be diagnosed, a person must have: Post-exertional neuroimmune exhaustion according to the criteria described. – At least 1 symptom from 3 neurological impairment categories. – At least 1 symptom from 3 immune/gastrointestinal/genitourinary impairment categories. – At least 1 symptom from energy metabolism/transport impairments categories. (More information about the symptoms in these categories can be found in a discussion of the ICC criteria by ME Research UK) Under the ICC, a diagnosis should be made when the clinician is satisfied that the patient has ME, rather than being constrained by a specific timeframe. | Any active medical condition that may explain the presence of chronic fatigue with examples including multiple sclerosis, Lyme disease, and Lupus erythematosus. This criteria also lists “non-exclusionary disorders” These include co-occurring disorders that do not adequately explain fatigue such as anxiety disorders, and fibromyalgia. |
| The 2015 IOM diagnostic criteria for ME/CFS. | |
| Requirements for a diagnosis | Exclusionary conditions: |
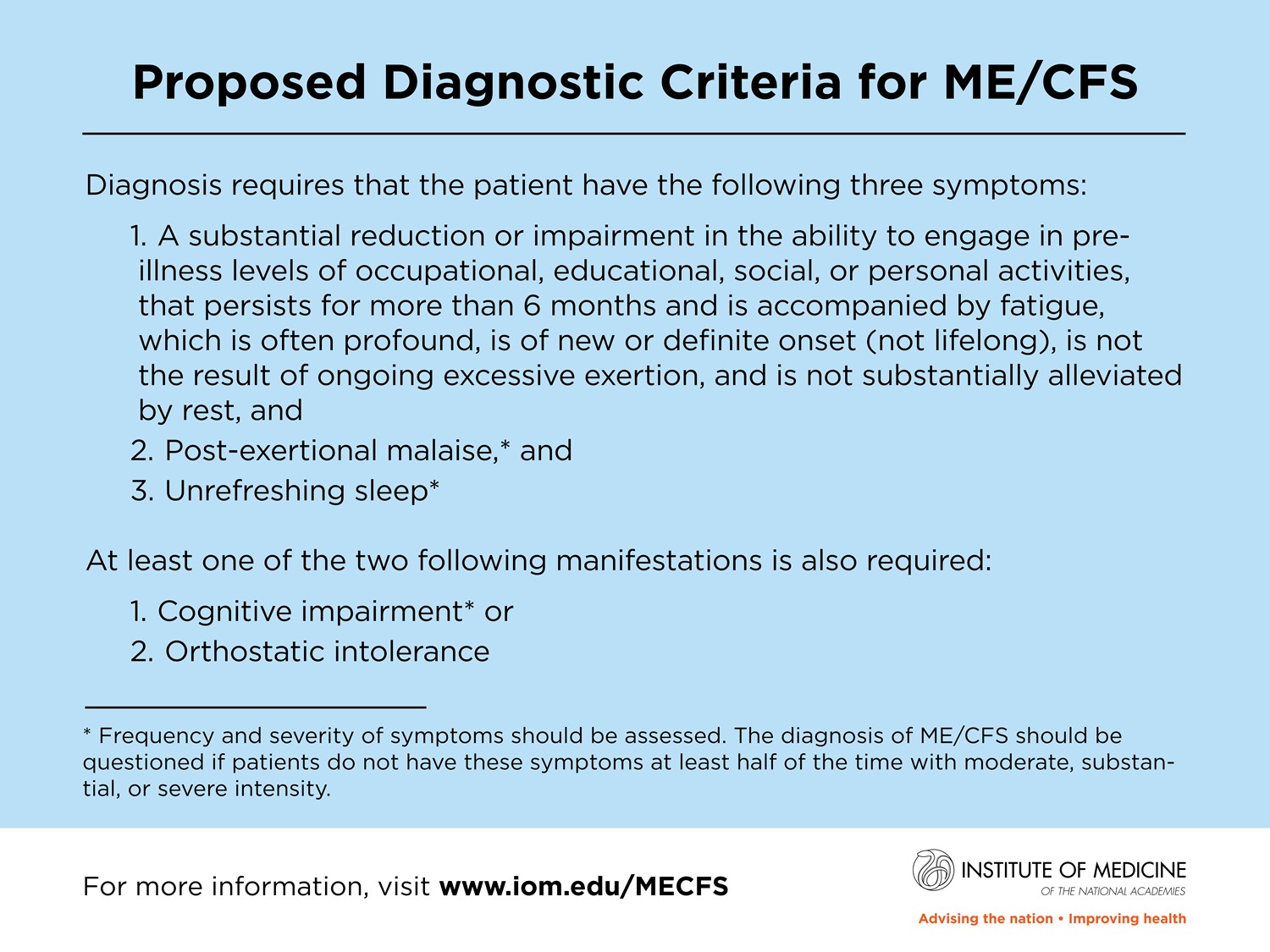
| Symptoms required for a diagnosis: Three symptoms and at least one of two additional manifestations are required for diagnosis. The three required symptoms are: A substantial reduction or impairment in the ability to engage in pre-illness levels of activity that lasts for more than 6 months, is accompanied by fatigue that is often profound, of new onset (not life-long), not the result of ongoing or unusual excessive exertion, and not substantially alleviated by rest. Post-exertional malaise (PEM).Unrefreshing sleep. The additional manifestations are: Cognitive impairment Orthostatic intolerance A diagnosis of ME/CFS should be made when symptoms last more than 6 months – although the on their website, the CDC note that: “A diagnosis of ME/CFS requires at least 6 months of illness. However, children and other patients should be seen by doctors and get support as soon as they become ill.” | None stated. |
As these diagnostic criteria rely on the child or young person’s self-reporting of symptoms or a description of symptoms from the child’s parent(s) or caregiver, additional factors must also be taken into consideration:
- Children and young people cannot always accurately describe their symptoms or how they feel.
- A child may describe their symptoms differently from how a parent or caregiver would describe them.
Research recommends that parent/caregiver report(s) and self-report of the child or young person should both be obtained to provide “a more complete understanding” of the child’s health.
Importance of an accurate and timely diagnosis of ME/CFS in children and adolescents
A commentary by Geraghty and Adeniji published in 2019 highlighted the importance of accurate and timely ME/CFS diagnosis in children and young people. In this paper, several key points were highlighted:
- Correct identification of ME/CFS is vital for children and young people so that “they might receive a speedy diagnosis and appropriate medical care and social support”.
- Accurate diagnosis of ME/CFS is essential for improving the accuracy of prevalence estimates for the disease.
- Misdiagnosis can lead to either under- or over-estimation of prevalence.
- Misdiagnosis in children and young people has “profound implications”.
- False positives (being given a diagnosis of ME/CFS when the child does not have it) can lead to improper intervention and treatment
- False negatives (not being given a diagnosis of ME/CFS when in fact the child does have the disease) can lead to the child not receiving the care they require.
The implications of inaccurate, and delayed ME/CFS diagnosis on education were also commented on in a paper by Peter Rowe and colleagues published in 2017 which stated:
“Many families have followed a long and circuitous route to diagnosis and the young patient can be months or years behind in school by the time a diagnosis is reached”.
It is also important to recognise that even when a diagnosis of ME/CFS is in place, the child or young person will need ongoing support such as educational accommodations, and due to the fluctuating nature of the disease, the level of support required may change over time.
Are there differences between ME/CFS in adults and the disease in children and young people?
While it is said that the core symptoms of ME/CFS – PEM, fatigue, unrefreshing sleep, and cognitive difficulties, are the same in both adults and children, some differences between the two age groups have been observed.
Research has suggested that ME/CFS prognosis – the expected course of, and chance of recovery from a disease, may be better in children than adults with the disease. However, as there have been few well-designed longitudinal studies – those that investigate a disease over a period of time, on the prognosis of ME/CFS in children and adolescents, it is hard to draw any firm conclusions.
The CCC for ME/CFS states that the disease may progress more slowly in children than in teenagers or adults, and the ICC criteria report that “Children can be very severely afflicted but those whose symptoms are of mild to moderate severity generally are more likely to have them go into remission than adults.”
There may also be differences in the symptoms experienced – the Centers for Disease Control and Prevention (CDC), report that compared with adults with ME/CFS, children with the disease may:
- Have more sleep problems such as difficulty falling or staying asleep, daytime sleepiness, and intense and vivid dreaming.
- Be more likely to have orthostatic intolerance – especially in girls who are post-puberty, headaches, and stomach pain.
- Be less likely to have joint and muscle pain.
It is also important to note that there may be differences in how ME/CFS presents before and after puberty. David Bell – a retired American doctor who had a practice in General Medicine and Pediatrics, states that “children below the age of 8 or 9 do not have the symptom pattern of adolescents past puberty”.
Summary
There is little research investigating ME/CFS in children and young people, and that which does exist is skewed towards biopsychosocial research, and often limited by the use of differing diagnostic criteria, and methods to obtain a diagnosis.
Although we do not know exactly how many children and young people have ME/CFS, it has been found that those with the disease may be experiencing inadequate health care. For example, a British Paediatric Surveillance Unit study – published in March 2024, identified several shortcomings in the management of children and young people with suspected severe ME/CFS, concluding that:
“Full investigation is frequently incomplete in children and young people with suspected severe ME/CFS and recommendations for referral and management are poorly implemented, in particular the needs of children and young people who are unable to leave their home might be poorly met.”
It is evident that ME/CFS in childhood impacts on education; school absences for ME/CFS are common and often prolonged – in fact, one UK study published in 1997 found that ME/CFS was the most common cause of long-term school absence. Additionally, as the diagnostic process is not straightforward and often long children with ME/CFS may not have a diagnosis. David Bell notes that ME/CFS diagnosis rates in children must be improved – without a diagnosis, school absences may be recorded as truancy.
It is essential that access to education is improved for children with ME/CFS – Bell highlights that healthcare professionals must work with education providers to ensure that children with ME/CFS receive the adjustments they need to be able to continue learning; for example, home tutoring scheduled at a time of day when ME/CFS symptoms are mildest.
There also appear to be differences in ME/CFS before and after the onset of puberty – with the risk of developing ME/CFS increasing after puberty, especially in females. Few studies have investigated why this is the case in detail, meaning more research is needed.
Conclusion
Overall, more research is needed to understand ME/CFS in children and young people, particularly that which aims to improve diagnostic procedures, health care, and access to education, and that which considers the impact of puberty on the risk – and symptom profile, of the disease.



{kind=link}